Funmilola A Ayeni1 ![]() ,
Bamidele T Odumosu2
,
Bamidele T Odumosu2
For correspondence:- Funmilola Ayeni Email: Fa.ayeni@ui.edu.ng Tel:+2347036138816
Received: 30 October 2015 Accepted: 12 June 2016 Published: 30 September 2016
Citation: Ayeni FA, Odumosu BT. False identification of other microorganisms as Staphylococcus aureus in Southern Nigeria. Trop J Pharm Res 2016; 15(9):1941-1945 doi: 10.4314/tjpr.v15i9.19
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: Staphylococcus aureus is the causative agent of many infections and the advent MRSA has drawn much attention to it. However, some organisms have been noted to be wrongly identified as S. aureus through phenotypic identifications leading to wrong treatment of infections. This study is therefore undertaken to evaluate the rate of false identification of other organisms as S. aureus in Southern Nigeria.
Methods: 507 microorganisms which have been previously identified as S. aureus in 8 States in Southern Nigeria through characteristic morphology on blood agar, Gram staining, growth and fermentation on Mannitol Salt Agar and coagulase formation were collected. All the isolates were identified in this study through sequencing of 16S rRNA and detection of spa gene. The percentages of true and false identities were determined.
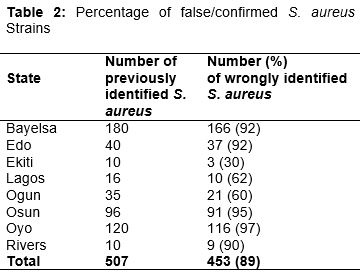
Results: Of the 507 isolates previously identified as S. aureus, only 54 (11 %) were confirmed as S. aureus while the rest were coagulase negative Staphylococci (85 % misidentification rate), Bacillus sp. (12 % misidentification rate), and Brevibacterium sp. (3 % misidentification rate).
Conclusion: A high rate of false positive identification of S. aureus which could lead to the misuse of antibiotics in emergency situation has been identified in this study. The use of standard methods for the identification of S. aureus at all times is highly recommended.
Introduction
Staphylococci are Gram-positive salt tolerant and spherical shaped bacteria. They are classified as coagulate positive (e.g Staph intermedius), Staphylococcus aureus and coagulate negative (e.g S. epidermidis, S. heamolyticus, S. capitis, S. saprophyticus). Some staphylococci are the causative agent of boils or septicemia infections and they have been reported as the leading cause of bacteremia, surgical wound infections and infections of bio-prosthetic materials in the United States; they are the second leading cause of nosocomial infections overall [1].
S. aureus is the most common species of staphylococci to cause infections. It colonizes healthy individuals and causes severe infection in hospitalized patients. About 20 % of the human population are long-term carriers of the bacterium [2] which has been implicated as a causative agent in acute food poisoning episodes, toxic shock syndrome, impetigo, scalded skin syndrome, cellulitis, folliculitis and furuncles [3]. Methicillin-resistant S. aureus (MRSA) is responsible for several difficult-to-treat infections in humans. MRSA is a serious threat to hospitalized patients globally and it now represents a challenge for public health [4]. Despite extensive infection controls, the emergence of MRSA has posed a serious therapeutic challenge and make S. aureus a serious pathogen warranting attention. In general the early diagnosis and treatment of infections caused by bacteria remain a major clinical challenge [5].
Identification of S. aureus is generally based on conventional phenotypic methods, encompassing culture and growth patterns on specific media. Growth and production of yellowish colonies on mannitol salt agar (MSA) is used for the selective isolation of S. aureus and as a characteristic for the differentiation of coagulase-positive staphylococci from coagulase-negative staphylococci (CNS) [6]. In the coagulase staphylococci differentiation method, the isolate is cultured on mannitol salt agar, which is a selective medium with 7–9 % NaCl that allows S. aureus to grow, producing yellow-colored colonies as a result of mannitol fermentation and subsequent drop in the medium's pH. S. aureus is catalase-positive (-catalase producer) and it is able to convert hydrogen peroxide to water and oxygen, which makes the catalase test useful to distinguish staphylococci from enterococci and streptococci. Ryan and Ray [7] observed that the organism can be differentiated from most other staphylococci by the coagulase test because most other Staphylococcus species are coagulase-negative.
Anecdotal evidence indicates that some microbiologists often rely on biochemical tests and growth on selective media to identify microorganisms. These methods can lead to wrong identification of some organisms and hence result in wrong prescription of antibiotics in which subsequently will lead to therapeutic failure [8]. The purpose of this study is to evaluate the level of false identification of S. aureus.
Methods
Study design
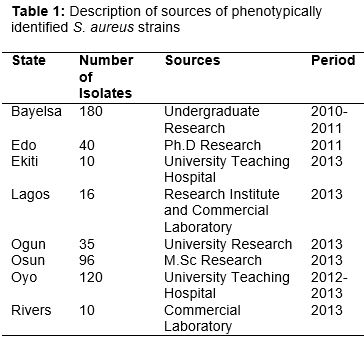
At least 10 previously identified S. aureus strains were collected from each of eight States in Southern Nigeria namely Edo, Rivers, Bayelsa, Ekiti, Osun, Oyo, Ogun and Lagos between 2011 and 2013. The organisms were preserved on agar slants at 4 oC and identified using molecular technique within 2 months of collections. A summary of the collection sources and numbers is presented in .
Methods of identification of S. aureus in the studied locations
The following phenotypic methods were previously used for identification of the strains as S. aureus across the States: (1) Characteristic growth and alpha haemolysis on blood agar, (2) Growth and production of yellow colonies on mannitol salt agar, and (3) Catalase positive test and coagulase positive reaction in slide test with human plasma.
Confirmation of identities of phenotypically identified S. aureus strains
Detection of spa gene and sequencing of 16S rRNA gene was used as standard identification methods for all presumptively identified S. aureus strains used for this study.
Detection of spa gene
The polymorphic X region of the staphylococcal protein A gene present in almost all S. aureus as described by Harmsen et al [9] was amplified for all isolated strains in a total volume of 50 μl by adding 1μl of a 1:500 dilution of genomic DNA, 1 µl of 25 Mm MgCl2, 1 µl of forward primer, 1 μl of reverse primer, 21 μl of water and 25 μl of AmpliTaq Gold® 360 Mastermix into a 0.2-ml PCR tube. Primers used were spa-1113F (5'-TAAAGACGATCCTTCGGTGAGC-3') and spa-1415R (5'-CAGCAGTAGTGCCGTTTGCTT-3'). A negative control (plain mastermix) and a positive control (from our laboratory's S. aureus collection) were included. Tubes were capped and placed in a Veriti Thermal Cycler (Applied Biosystems). Thermal cycling conditions included an initial 10 min at 95 °C followed by 32 cycles of 30 s at 94 °C, 30 s at 55 °C, and 60 s at 72 °C; and a final extension at 72 °C for 10 min. PCR products were resolved by agarose (1 %) gel electrophoresis previously stained with GelRed (Biotium Inc, Hayward, CA, USA) and run at approximately 40 mAmp for 45 min. The molecular marker used was a pUC mix Marker 8. The size of the PCR products was 400-600 bp for the spa gene.
Identification by partial sequencing of 16S rDNA gene
DNA was extracted using QuickExtractTM DNA extraction solution (Epicentre, Wisconsin) according to the manufacturer’s instructions. The extracted DNA was then used as a template in PCR amplification with primers, BSF-8 5`-AGAGTTTGATCCTGGCTCAG-`3, BSR-534 5`-ATTACCGCGGCTGCTGGC -`3 [10], in a 20 µl reaction consisting of 10 µl Master mix (RedTag, Sigma, Aldrich), 2 µl primers, 1 µl DNA and 7 µl water. The PCR conditions are 10 min of initial denaturation at 95 °C, followed by 45 cycles of annealing of 15 s at 95 °C, 30 s at 55 °C, 30 s at 72 °C followed by a single 7-minute extension at 72 °C and finally set on hold at 4 oC. The PCR products were analyzed on 1 % agarose gel in TAE buffer containing GelRed, run at approximately 40 mAmp for 45 min and visualized under UV light. These were purified and sequenced using standard procedures. Identification to species was performed by choosing the best match after searching individual 16S rRNA gene sequences against the EzTaxon-e server that contains comprehensive 16S rRNA gene sequences of taxa with valid names [10].
Results
Of the 507 isolates previously identified as S. aureus only 54 (11 %) were confirmed as S. aureus. The distribution of the rate of false identification of the organism is provided in . Coagulase negative staphylococci (CoNS, 85 % misidentification rate), Bacillus sp. (12 % misidentification rate), and Brevibacterium sp. (3 % misidentification rate) were the organisms found to be most frequently misidentified as S. aureus.
Discussion
Reliable identification of S. aureus is of major concern in clinical microbiological diagnostics [11]. In the current study, we found that only 11% of isolates previously identified as S. aureus were confirmed as S. aureus. Coagulase negative staphylococci (CoNS) were the organisms most often misidentified as S. aureus followed by Bacillus sp. and then Brevibacterium sp.
Partial 16S rRNA gene sequence analysis has served well as a gold standard method for the identification of a variety of microorganisms including Staphylococcus spp. due to large reference databases [12]. Bacillus sp. and Brevibacterium sp. all grew on MSA with yellow colonies and most strains causes haemolysis on blood agar. These are characteristics often used to identify S. aureus in Nigeria and thereby leading to gross misidentification of these strains. Because of their ubiquity and low virulence, CoNS have generally been considered to be non-pathogens or simple contaminants and therefore less attention is paid to their proper identification [13]. However, CoNS are becoming more involved in various infections. Brevibacterium species are pleomorphic, Gram-positive bacteria, and are difficult to identify due to their morphological and physiological similarity to members of genera such as Arthrobacter, Caseobacter, Corynebacterium and Rhodo-coccus. Rattray and Fox [14]. Brevibacterium linens is ubiquitously present on the human skin, where it causes foot odour. Bacillus is a genus of Gram-positive, rod-shaped bacteria and a member of the phylum Firmicutes. Bacillus species will test positive for the enzyme catalase when there has been oxygen used or present [15].
The definitive test for S. aureus versus other Staphylococcus species is the test for coagulase production. When identification is based solely on this phenotypic characteristic, accurate identification could depend on the plasma used for the coagulase test. More consistent results could be obtained with BBL plasma than with the Difco plasma [11]. However, human plasma are usually used in Nigeria.
Rapid and reliable species identification of these organisms is essential for accurate diagnosis and prompt effective treatment of infections. Staphylococcus aureus is a major cause of both healthcare associated and community acquired infections throughout the world and the major problem associated with MRSA infection lies in identification of strains. In a study conducted in Libya in 2010 on rate of misidentification of MRSA in Libya, Of the 170 isolates examined, 86 (51 %) were confirmed as MRSA (i.e. 49 % were misidentified as MRSA) [16]. Charyulu et al [17] also observed 10 true S. aureus strains out of 106 identified as S. aureus in India.
Since staphylococci are components of the normal flora of many body sites, it is important for diagnosis, treatment, and epidemiology to be able to recognize S. aureus as the etiologic agent of suspected staphylococcal disease. [11]. Accurate identification of S. aureus isolates is crucial for the correct management of infections, Due to the advent of MRSA, clinical laboratories will have an increasing need for rapid and reliable methods of identifying the causative organisms at least at the species level.
In Nigeria, researchers and clinical microbiologists rely on fermentation of mannitol and coagulase production for identification of S. aureus. However, Notarnicola et al [11] stated that the standard combination of coagulase production, DNase production, and mannitol fermentation cannot be depended on to give accurate identification of S. aureus. The results of this study indicate that some of the tests currently being used in identifying S. aureus in Southern Nigeria lead to the misuse of various classes of antibiotics and contribute to increased resistance.
Conclusion
The results of this study indicate that there is high false positive identification of S. aureus in Southern Nigeria. This could lead to the misuse of various classes of antibiotics in emergency cases and thereby contribute to increased resistance. Education of microbiologist working in hospital microbiology laboratories in Southern Nigeria is vital.
Declarations
Acknowledgement
References
Archives


News Updates